Physician Leaders I Admire – Bob Wachter, UCSF
Recently while following my twitter feed, I noticed the following from an associate editor from The Health Care Blog who quoted Dr. Lucia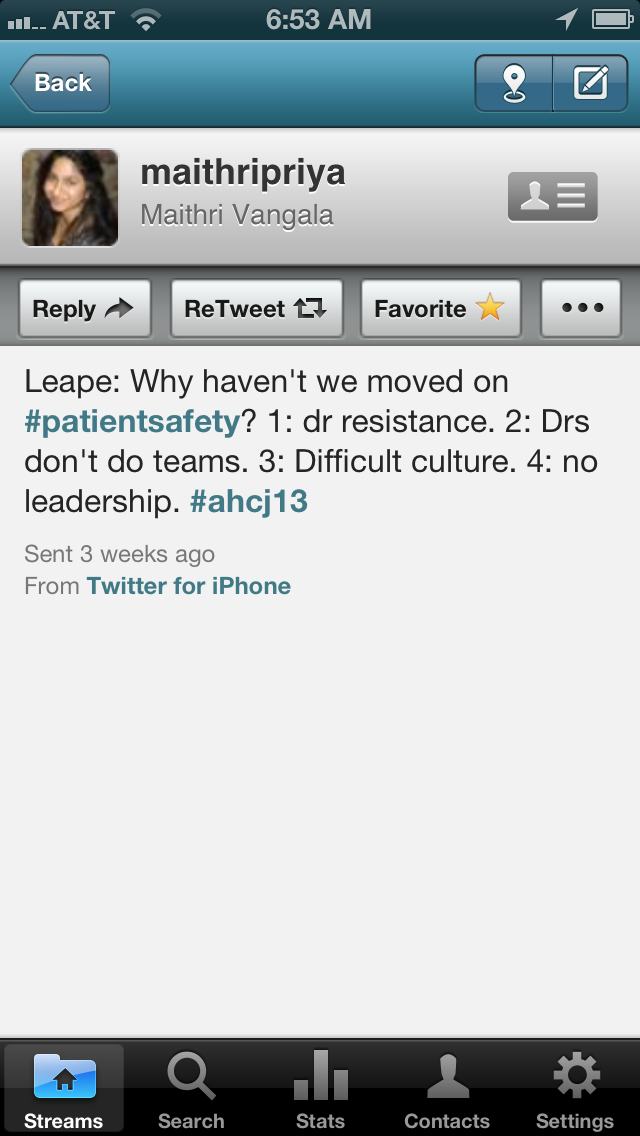 n Leape, Harvard School of Public Health. Dr. Leape wondered why the patient safety movement hadn’t moved. He noted four reasons:
n Leape, Harvard School of Public Health. Dr. Leape wondered why the patient safety movement hadn’t moved. He noted four reasons:
- Doctor resistance
- Doctors don’t do teams
- Difficult culture.
- No leadership.
Though I did not attend the conference where Dr. Leape spoke, the answer seemed pretty obvious. To solve the problem you need leadership. It is leadership that defines the culture, whether teamwork is valued, and whether change occurs.
The reason health care has not moved forward quickly enough simply because there has been a void of physician leadership across the entire health care system. There have been plenty of initiatives to improve patient safety over the past decade since the Institute of Medicine “To Err is Human: Building a Safer Health System“, but as stories demonstrate many of these initiatives are taking hold in pockets of excellence where strong physician leadership is making a difference. Other hospitals and health care systems, tragically are not doing enough or moving quickly enough to make change.
So who are the physician leaders leading the change? Here is one physician leader I admire.
Dr. Bob Wachter, UCSF, the father of the hospitalist movement, patient safety advocate, and brilliant systems thinker, among many other titles, first appeared in my life via an article in my 2004 alumni magazine from the University of Pennsylvania. The article, The Talking Cure – A More Collaborative Culture in Health Care Could Reduce Medical Errors — and Save Lives”, was a brilliant excerpt from his book Internal Bleeding: The Truth Behind America’s Terrifying Epidemic of Medical Mistakes. The excerpt unfolds immediately into the frenzied controlled chaos of a code blue. The code team leader, a resident physician who had been already accepted into an ICU fellowship, calls off the code blue after discovering the patient was no code, a do not resuscitate (DNR) order.
As the code team left, the young nurse, a recent graduate and the individual who called the original code blue, thought it odd that no one had mentioned that her patient’s code status was changed from full code (do everything to resuscitate) to DNR. As she was cleaning up she was stunned to discover that the code team leader had pulled the wrong patient chart. She noted that the patient still had a faint pulse.
The patient the code team had stopped resuscitating was actually full code. The patient had wanted everything done. The code team was called back again, but failed to revive the patient.
As Dr. Wachter notes in the piece:
- Whether it is in the OR or at a Code Blue, medicine has not done a great job in delimiting roles and responsibilities, fostering teamwork, and reflecting on the interpersonal relationships that often define success and failure. Even after a Code Blue, there is virtually never a formal debriefing—the team just breaks up and wanders off, to resume their regular duties. When CPR is unsuccessful, which is most of the time, we may ask ourselves individually why we failed (“Should I have given another dose of epi?”), but our failure as a team is never considered.
- Aviation is often held up as a model of how professionals working in high-risk, high-demand, high-tech environments can collaborate successfully without letting hierarchy, tradition, or prejudices get in the way. While pilots are lauded for their receptiveness to collaboration, physicians are seen as poster-boys for inflexibility. The unflattering comparison has some merit. One study compared the attitudes of flight crews regarding teamwork to those held by surgical teams. Nearly half the surgeons felt that junior team members shouldn’t question the decisions of the senior physician. In contrast, 94 percent of airline cockpit crews rejected this sort of hierarchy—possibly because when the captain makes a mistake, he and his entire crew go down as well.
- Unfortunately, the doctors who discourage such crosstalk are the kind who need it most. In the survey just described, 70 percent of attending surgeons agreed that, “even when fatigued, I perform effectively during critical times.” Among pilots, only a quarter self assessed as such.
In this 2004 article, nearly a decade, ago, Dr. Wachter calls out exactly what Dr. Leape notes is missing – a collaborate culture, teamwork, and a willingness to learn which are perfect foils for difficult culture, doctors don’t do teams, and doctor resistance.
Learning from others is important. Dr. Wachter advocates blameless root cause analysis, which is essentially borrowed from aviation and other highly reliable organizations. To investigate mistakes we need to look at the dynamics of the team as well as the environment the team operates in. We need to look at cultural and system issues. These can be addressed by physician leadership.
Yet in health care, we always think we are different. Protocols, checklists, and safeguards that work elsewhere don’t apply to us. Instead of acknowledging that we too are human and the cognitive errors and lapses that occur are simply a consequence of being human, somehow is irrelevant when it applies to providing medical care. So when there is a medical mishap and the outcome is less than ideal, the health care mindset is that someone didn’t do his job or wasn’t conscientious enough. Too often, we are too harsh on the individual who is the last person who could have stopped the bad outcome. Sometimes, the consequences for the individual are severe.
Dr. Wachter has noted that sometimes doctors can take blameless root cause analysis in “blaming the system” too far, when on further inspection the error is clearly on the individual. As a leader, he calls that out as well.
Having a physician call out another physician is not easy. Modeling the type of behavior we want is not easy.
It is ho wever necessary if health care is to move forward.
wever necessary if health care is to move forward.
Dr. Wachter is a physician leader I admire, follow his blog and tweets, and also hope to emulate.
Shortly after reading the Penn Gazette excerpt, my father had a retinal detachment which did not heal properly. It was the consequence of a medical error, specifically an error of omission. It was the second time my family had such an event. The first was avoided by pure luck. It was this second mishap that I felt compelled to write. But, of course, I have no experience in book publishing. I checked out books from the library, figured out how to write a proposal, started to writing my book and published some opinion pieces in the Sacramento Bee and the San Francisco Chronicle.
However, it would be helpful to learn from someone who already published a book. A physician author.
So I emailed Bob with the simple subject heading – From Davis Liu – UPenn Class of 1993.
Despite his incredibly busy schedule, Bob was willing to take an hour long phone call from a complete unknown (aside from being Penn alumnus) describing his experience on book publishing. He replied to my periodic emails. Listening for new voices and exploring possibilities even if an unknown quantity, mentoring future leaders by giving time, and providing support when needed – these are signs of leadership.
Bob was kind enough to write a testimonial for my first book:
“Our health care system is becoming increasingly complex and confusing. More than ever, staying and getting well requires that patients be informed about their care. This thoughtful and engaging book is all you need to get the right care – reading it is like having a doctor in the family.” – Robert M. Wachter, M.D., author of Internal Bleeding: The Truth Behind America’s Terrifying Epidemic of Medical Mistakes, Professor and Associate Chairman, Dept. of Medicine, University of California, San Francisco.
And Bob is further impacting the next generation of hospitalists and physician leaders with his recent cameo in ZDoggMD’s video celebrating hospitalists (which is “a made up word”).
So, Bob Wachter is a physician leader I admire.
Which physician leaders do you admire?
 Get important exclusive advice and tips on how to save money while staying healthy.
Get important exclusive advice and tips on how to save money while staying healthy. Learn how to make intelligent choices in America's Healthcare System.
Learn how to make intelligent choices in America's Healthcare System.